

〽️Service Stats & Updates
As of Monday April 27, 2026...
20,985 samples analyzed
Serving 199 harm reduction programs
Reaching 296 counties in 44 states
511 unique substances identified
Nab's Testimony to US House of Representatives Health Subcommittee
Recently, Dr. Nab Dasgupta went in front of Congress to testify about the unintended consequences of scheduling xylazine — and why getting drug policy wrong can make a dangerous situation even worse. Check out his written testimony, watch the web recording, or catch it on YouTube! We are all so proud!
⚠️Bots Using Our Data
We've heard your concerns about third parties scraping our drug results site and making apps, or using the data for AI training. We have revised our Data Use & Protection policy to make it explicitly clear that these purposes are not allowed.
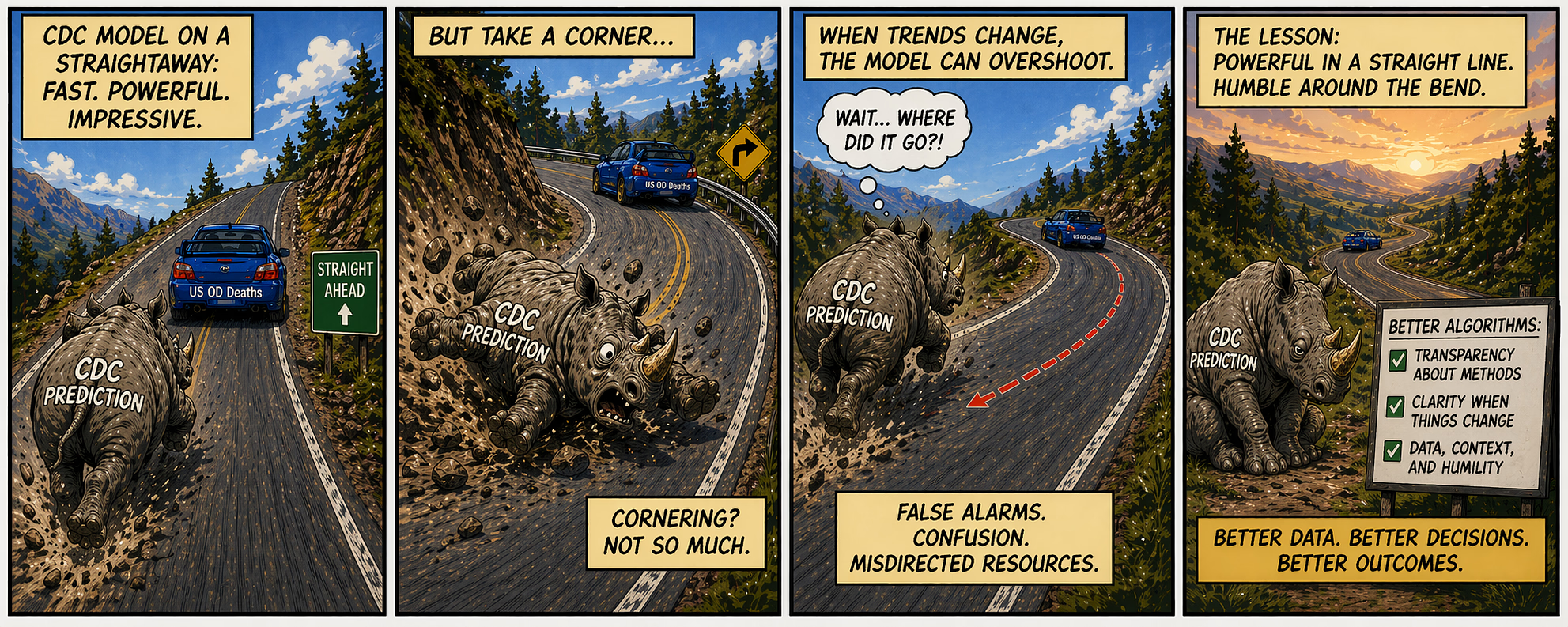
📉 Department of Data
What's going on with CDC's overdose prediction algorithm? It works great when trends are moving in a line (up or down). But when rates turn a corner and start to decline nationwide like in 2023, the model overshot. And, now with OD acceleration in some states, it's poised to underestimate.
The 2025 Drug Overdose Spike That Wasn’t: Neither Politics nor Data Errors Explain the Anomaly
We also want to point out this new CDC resource that shows the prevalence of cocaine, fentanyl, heroin and methamphetamine in clinical urine drug test samples collected by Millennium Health labs.
👀 Have we seen cychlorphine?
Yes, we've been tracking the-molecule-currently-known-as cychlorphine since our first detection in August 2024. We haven't see it in NC samples, but if our service users suspect it, please note it down on the card. Cychlorphine is a minor concern relative to fentanyl because it currently doesn't make up even 1% of the illicit opioid supply. There are much more important and concerning things to pay attention to, namely medetomidine withdrawal heart attacks; it's not just about overdoses.
Human effect information is limited. You can see all the samples under it's proper name N-propionitrile chlorphine and summarized in this Live Report.
Naming of orphines is a mess. For example: N-propionitrile chlorphine = chlorphine = cychlorphine and "SR-17018" = 5,6-Dichloro Desmethylchlorphine. We are working with NIST to standardize naming, but be aware that this is in flux.
Ibogaine: In light of last week's federal announcement on ibogaine, it's worth hearing from our friend Dimitri Mugianis who has more decades of experience with ibogaine and Bwiti in the US than just about anyone else. (Who was immortalized in this Law & Order SVU episode.) The main point? "Without additional resources, psychedelics like ibogaine can’t support recovery or mental health."
What we are actually worried about-
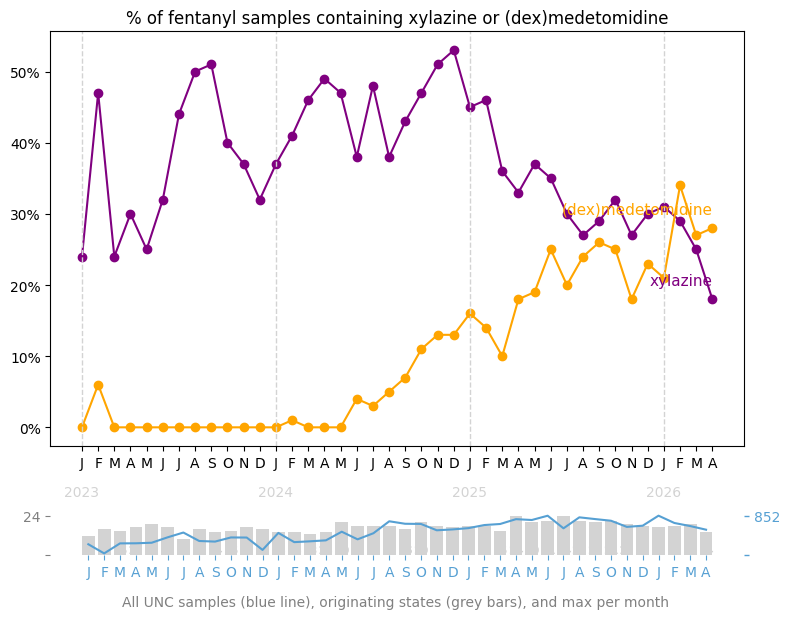
As expected, medetomidine is replacing xylazine in our samples. Good news, medetomidine doesn't cause horrific skin wounds. Bad news: Quitting cold turkey can give you a heart attack and land you in intensive care. In Pittsburgh, hospitals are filling up – not with overdose – but with people who tried to stop using what they thought was fentanyl but had medetomidine. It's a complicated weeklong hospital intensive care stay with 14 medications to treat these drug-induced heart attacks. Yet, medetomidine is a REALLY IMPORTANT medication in hospitals to sedate babies on respirators and adults after surgery.
At Prevention Point Pittsburgh, where medetomidine is replacing fentanyl, they are telling folks who want to quit to skip the methadone/buprenorphine clinic and go wait in the hospital emergency room. Life threatening withdrawal doesn't happen to everyone, but can start 2 to 26 hours after last use. This will blow up all the MAT and telehealth services that you all worked so hard to build! This makes "just say no" potentially lethal advice, and abstinence-based residential treatment programs should be ready to provide transport to the hospital for new patients when withdrawal hits.
Pay attention. This is the real drug story of the month, not cychlorphine or ibogaine. How do we keep it out of our communities? Can test strips empower people who buy drugs to push back on suppliers? We need to get creative, and we need to do this now.
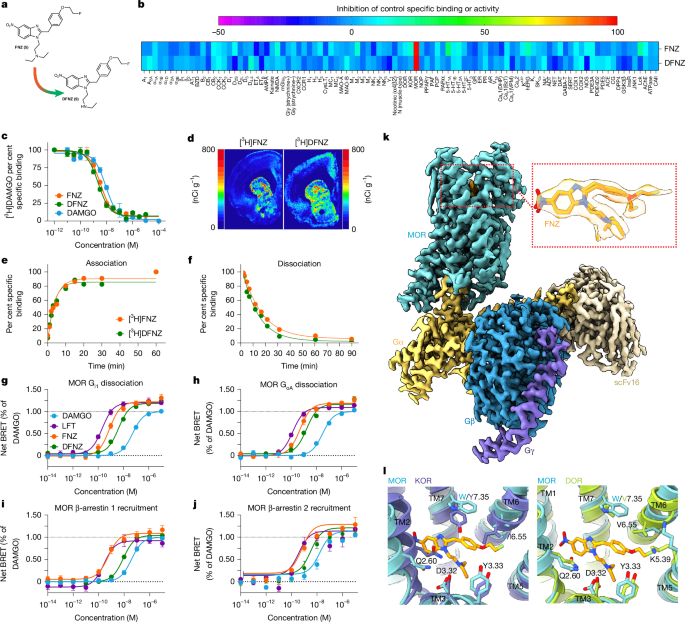
Heard of DFNZ?
No, it's not Drug-Free New Zealand. 🇳🇿 A NIDA-led team of scientists from the US and Spain discovered a new molecule that could just be the holy grail in pain management. It's a high-efficacy "superagonist" at the µ-opioid receptor (e.g., great pain relief in animal models), with markedly less respiratory depression, tolerance, withdrawal, and reinforcement than standard opioid analgesics. Guess what? It's derived from a nitazene! N-desethyl-fluornitrazene. Yeah, that same class of new synthetic opioids that the media has been over-hyping as the next dangerous thing in the illicit drug supply. But, the sad thing is it may never make it to medicine cabinets. Why? Because Congress is poised to permanently ban ALL nitazenes, including DFNZ. 'Tis pity to be so shortsighted.
✈️ Out and About

Jesse Bennett 🖤
We bid a sad farewell to Jesse Bennett, former head of the NC Harm Reduction Coalition, who passed away on April 15th in Raleigh, NC. An NC State graduate, and dad of two two kids, who helped shepherd our movement in the South through a very influential period. See his bright smile in this photo album. Godspeed, friend. You did a world of good!
📖 Reading Room
Read up on articles we found engaging or maybe watch a video about-
Academic Emergency Medicine: Naloxone Administration in Relation to Fentanyl, Xylazine, CNS Depressants, and Stimulants Exposure After Suspected Opioid Overdose
Watch this fascinating interview with one of the brightest minds in international drug policy- Ann Fordham. She recently left her post at IDPC after 17 years. This is a reflection on the state of drugs globally over the last two decades. Produced by our friend István
Comms Resources from Prison Policy Initiative: We recently learned about this great series of guides for data-based messaging from Wendy Sawyer at the Prison Policy Institute. Here's their writing guide, advocacy toolkit, guide to managing and organizing public data. Our fav was this guide to designing effective visuals.
Lighter content- Fast Fish Cocaine: The illegal drug’s main byproduct, benzoylecgonine, caused more robust effects than cocaine itself.
NY Times: How the Internet Became the ‘Cookbook’ of the Drug Trade
Syringes & War: One of the unintended consequences of the War on Iran is that countries like South Korea are experiencing a shortage of syringes. We don't know if this will impact US hospitals and SSPs, but anything plastic in the supply chain is up for disruption. We haven't heard of this affecting the US yet, but it would be worth checking with suppliers if shortages are on the horizon.
The American College of Medical Toxicology (ACMT) supports the use of expired naloxone to reverse suspected opioid overdose in situations where unexpired drug is not available.
This is a clever and important paper from Caroline Copeland's team at Kings College London. Nitazenes disappear in post-mortem toxicology. When blood samples are handled in the standard manner for autopsy, common nitazenes have less than 10% detectability. This will be a huge problem for OD death data if/when nitazenes emerge in force in the US.
🤗 Opportunities for Impact
Job postings, conferences, proposals, and other events for you harm reduction baddies! If you have a job posting or event you'd like us to highlight, please be in touch.
Join ACDC for the seventh annual Alliance for Collaborative Drug Checking (ACDC) Virtual Learning Summit!
Durham NCHRC Drug Alert Bulletin: An example of what programs are doing to convey drug checking data to participants!
Edgecombe County Emergency Services is currently accepting applications for a Post Overdose Response Team (PORT) Community Paramedic!
UC San Francisco is hosting an OIDA symposium THIS May, check it out!
Welfare Research Inc., based in Long Island, NY is searching for a drug checking technician!
The Hair Study Recruitment study below will evaluate if environmental hair contamination can lead to positive hair drug tests and they are looking for volunteers!
Expired Test Strips
The shelf-life of BTNX xylazine test strips have been extended. Check lot numbers to be sure. Fentanyl test strips can also be used past expiration, but their limit of detection may shift- so that minuet amounts may be harder to detect.
📦 Service Updates
Thank you all for your continued partnership. We appreciate the important work you do in your communities!
- Samples are always voluntary, and individuals must have access to their results!
- Please do not share kits between programs-reach out to us if needed and the original kit owner will be responsible for the shipment/materials fee.
- Use only the materials and labels we provide and ship via FedEx only
- Do not add water to vials; if solution has evaporated (around 3 months), that’s okay, just contact us
- Be mindful of shipping timelines when ordering and returning kits
Data Cards Reminder
Please fill out data cards as thoroughly as possible. Knowing the expected substance helps ensure accurate lab analysis, and sensations data are critical for understanding changes in potency and composition in the drug supply.
Mailer Update (Effective May 1)
Starting May 1, there will be a $10 fee for additional mailers for all programs, including those in North Carolina. One mailer is provided per 5 kits. We do not want you holding onto 1-2 samples for an extended time but also you can send more than 5 samples back in a box if necessary! This change helps us cover rising material and shipping costs, and we appreciate your understanding.
Happy drug checking!
Thanks from the Opioid Data Lab team!
