
This was a consequential year for drugs and drug policy in the United States. Next year will be pivotal. The kind of opportunity for lasting change that comes along once in a few generations. Here's our top 4 trends and predictions for 2026:
- Generational shifts in drug preference among Gen Z suggest an enduring change away from opioids. Cannabis and psychedelic regulation will be hotly contested.
- Sedatives and anesthetics displacing fentanyl will increase dissatisfaction with the drug supply, reduce opioid exposure and decrease OD risk, but portend even more difficulty getting people into treatment.
- Geopolitics of drug production are poised to reconfigure who profits from the (drug) war, leading to market consolidation and alternate trade routes, as well as new substances and scapegoats. From the chaos, new drug market millionaires will be anointed.
- Cratering federal funding for treatment and prevention will put stress on states and local hospitals. Counties will feel pressure to divert opioid settlement funds. AI powers will forward government surveillance. Housing versus forced treatment will be a central debate.
The big picture is that the really positive gains from 2024 lent momentum to continued improvements in 2025. But we also may have missed a bit of an opportunity, distracted and underfunded this year, to turn the whole thing around. Maybe easing our foot off the accelerator, not hitting the brakes. Through this gap we see glimpses ahead of a worsening drug supply. Or maybe that's what the drug market would have done anyway.
Years of emphasis on treatment and harm reduction worked! Misguided experiments peeling these back have already showed how easily drug harms can re-emerge. As the drug supply is further destabilized, myopic obsession with just fentanyl, militarism, and short-term fixes drain away our rare opportunity to make lasting generational improvements. While underfunded and traumatized, the harm reduction workforce is remarkably resilient, and will once again be asked to do more than their share to protect our neighbors.
Buckle up! Below, we cover the biggest drug stories of 2025, and make the case why 2026 is poised to be a year of major change.
Overdose Trends
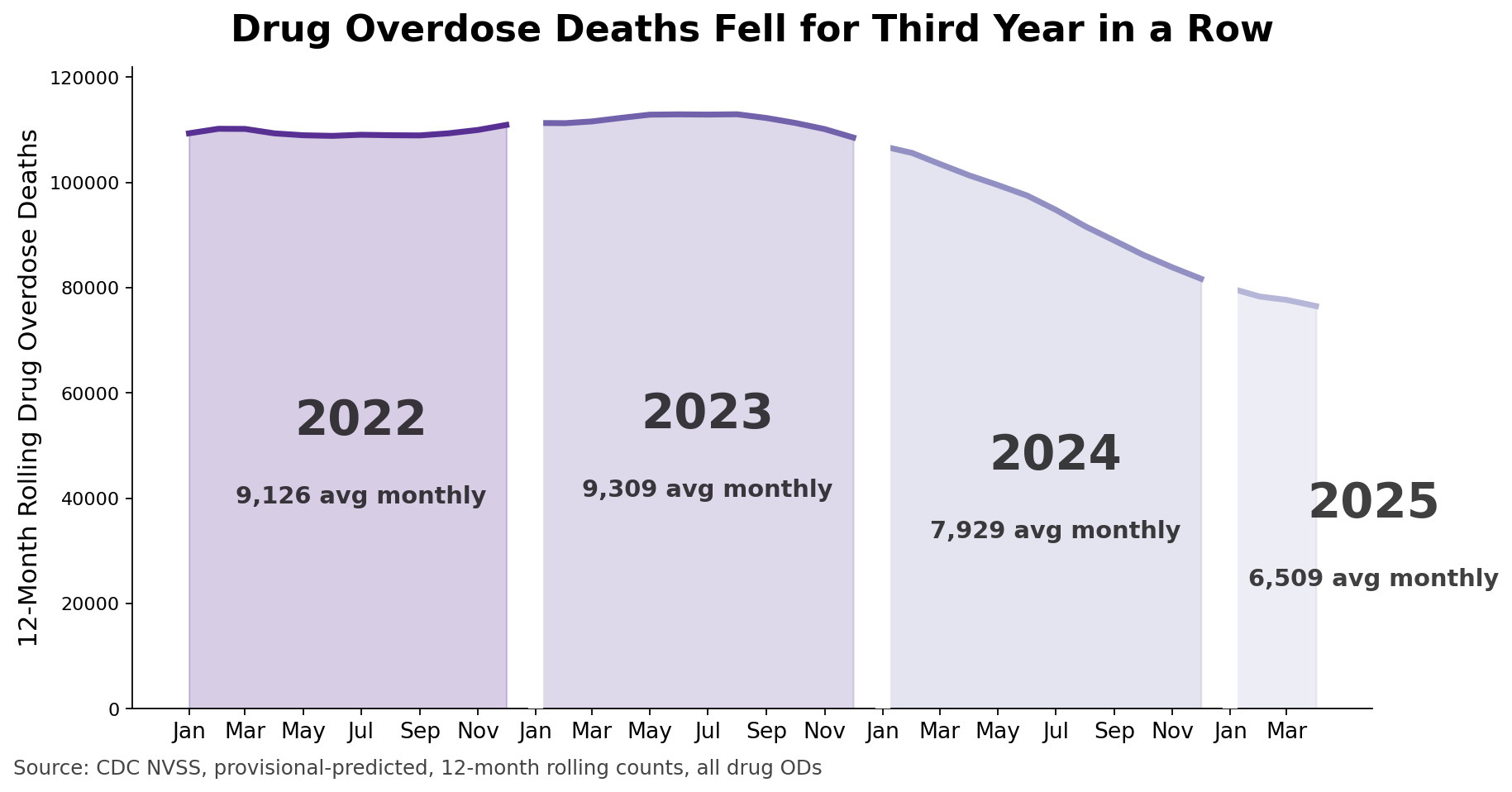
Earlier in the 2025 we learned that overdose mortality rates have been declining in the United States since 2021, and that all states trended downward by 2024. Different parts of the US experienced the neap and ebb tides of fentanyl as haphazard waves over the past half-decade. From the macro level to local, explanations for this decline consistently point to changes in drug supply, protective drug user behaviors, and interventions. OD deaths dropped in nearly all states by 20-30% from peak years. Nationally, we are roughly back to where we were pre-COVID, but still 4x higher than at the start of the century. We are still losing too many people we love.
According to the revised CDC provisional-predicted overdose death data, Peak OD in the USA was June 2023: 111,466. The most recent 12-month period available is April 2025 with 76,516 deaths. This would be a reduction of 31.3%, but we are still not sure how major methods changes in February 2025 affect interpretation. (More on this below.)
2025 Overdose Spikes
Yet, state and city data show that some places saw a transient increase in fatal and non-fatal overdoses in late 2024 and into the first half of 2025. The good news is that the jumps had largely quelled by late summer, resuming years-long downward trajectories. Expect annual year-over-year fatal OD rates for 2025 to show an overall decline nationally, but compared to previous years they will be attenuated.
Curiously, the early 2025 OD spikes didn't follow a clear pattern geographically. Milwaukee and Seattle saw an increase in fatal ODs in November 2024, the same month as Arizona. In San Francisco and statewide California the peak emerged in January 2025. Cleveland saw an increase in 1Q2025, and Seattle saw another peak in March. But over in New England (Connecticut, Maine) it was in 2Q2025, peaking in June. Here in the South, Kentucky also peaked in June, whereas North Carolina saw the bump a couple of months earlier in April. Random?? The fastest reporting locations consistently show a resumption in OD decline into the Fall of 2025. Some of those deaths are still under investigation, but even accounting for that lag, the overall picture seems to be of a transient surge in overdose deaths in the first half of the year, continued by a resumption of decline.
International Comparisons
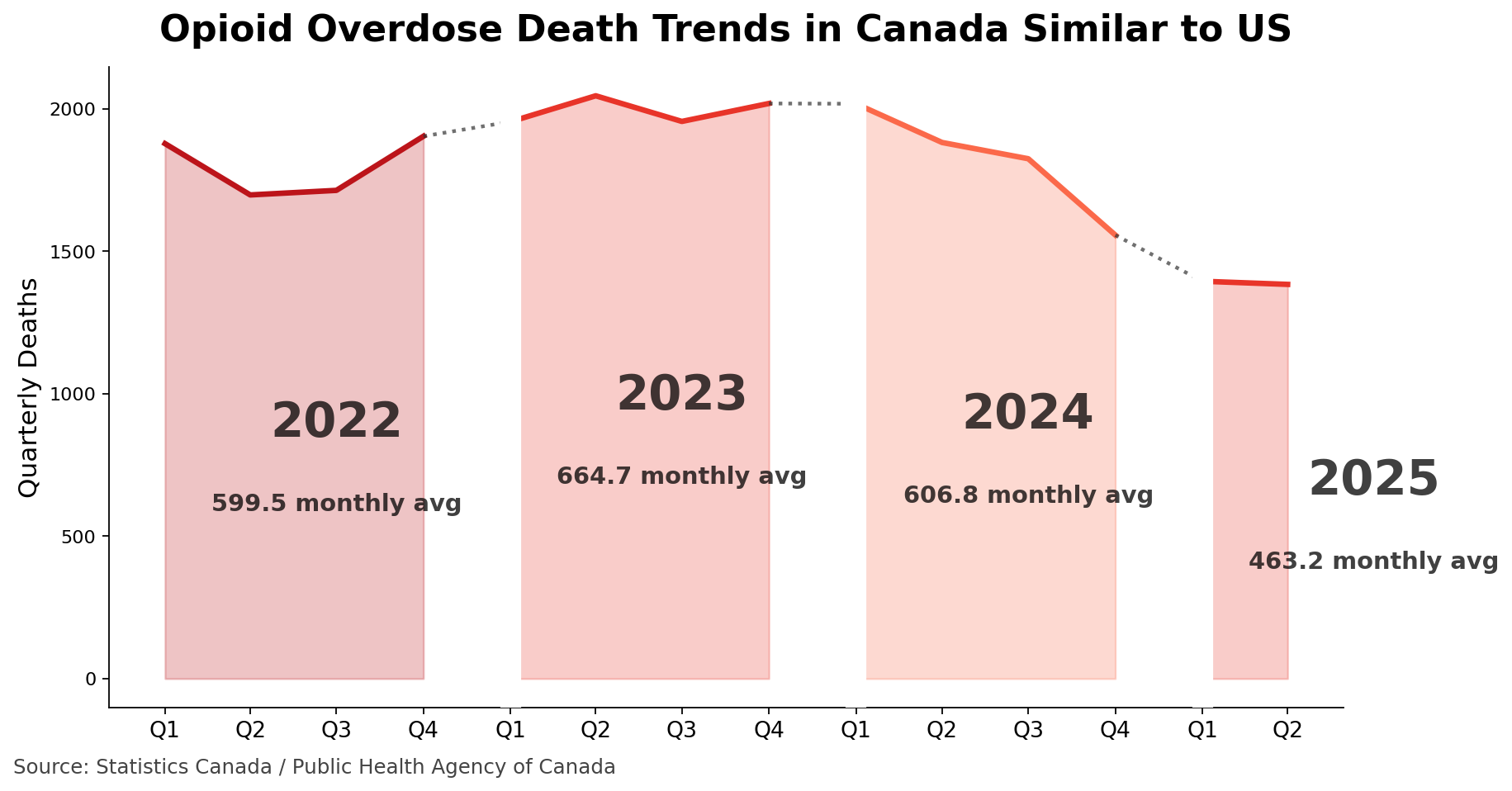
🇨🇦 Lest we think that what we are experiencing in the United States is a unique, let's take a look at similar opioid overdose mortality data from Canada. Fentanyl and its analogues made up the majority of opioid ODs, similar to the US.
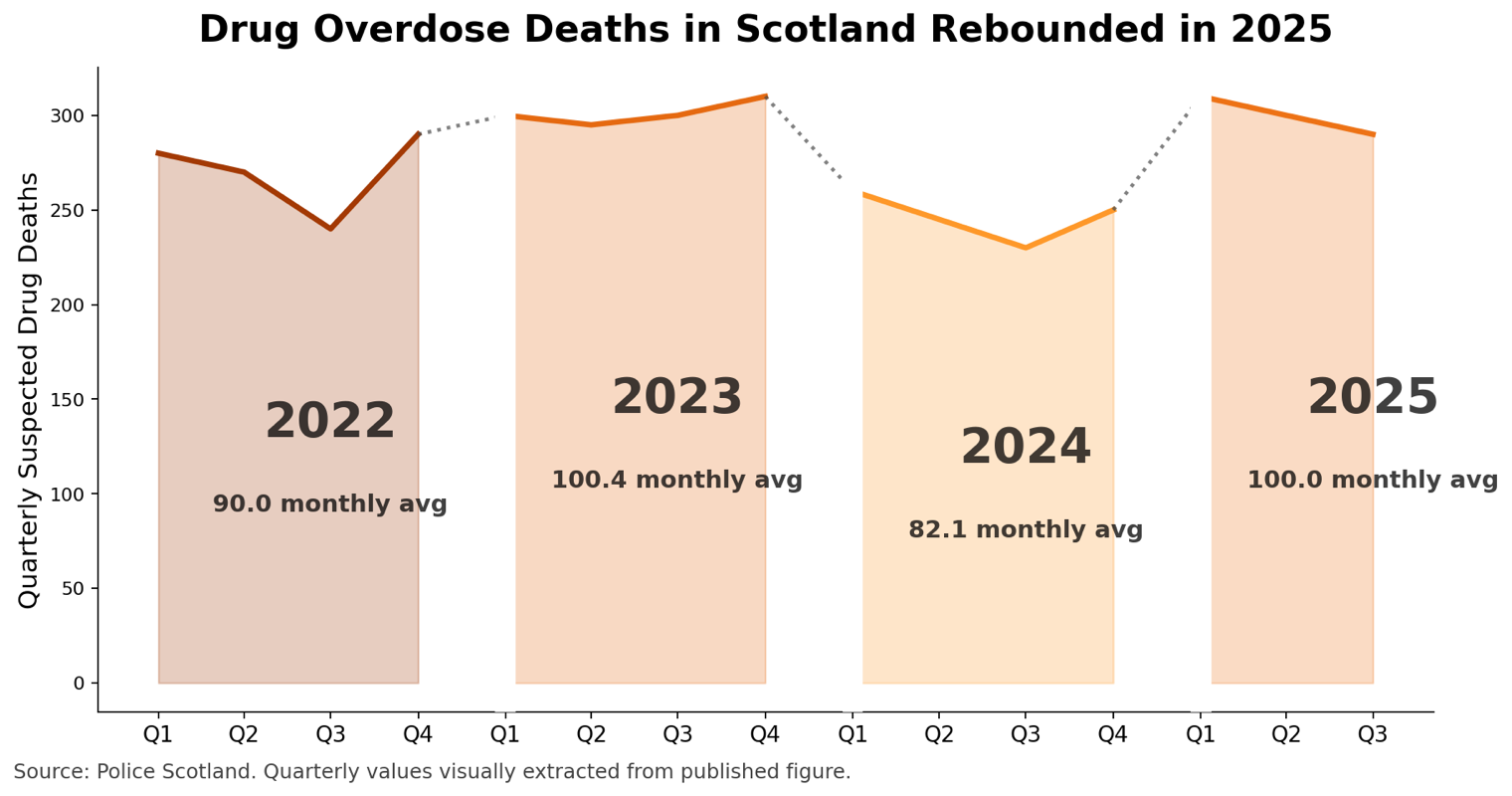
🏴 But in Scotland, we saw a different picture, with OD deaths rebounding in 2025. The most common drugs involved were methadone, heroin, and nitazenes. So, while there were different drugs involved from the US and Canada, the drop in 2024 was similar.
Generational Changes
In 2025 we also noticed intergenerational changes in opioid use and overdose, with (most of) Gen Z reducing their OD risk, along with a shift towards cannabis, psilocybin, MDMA, and ketamine. Also less alcohol.
Key to remember: 7-out-of-10 overdose deaths are happening in Gen X and Millennials. This is where resources need to go.
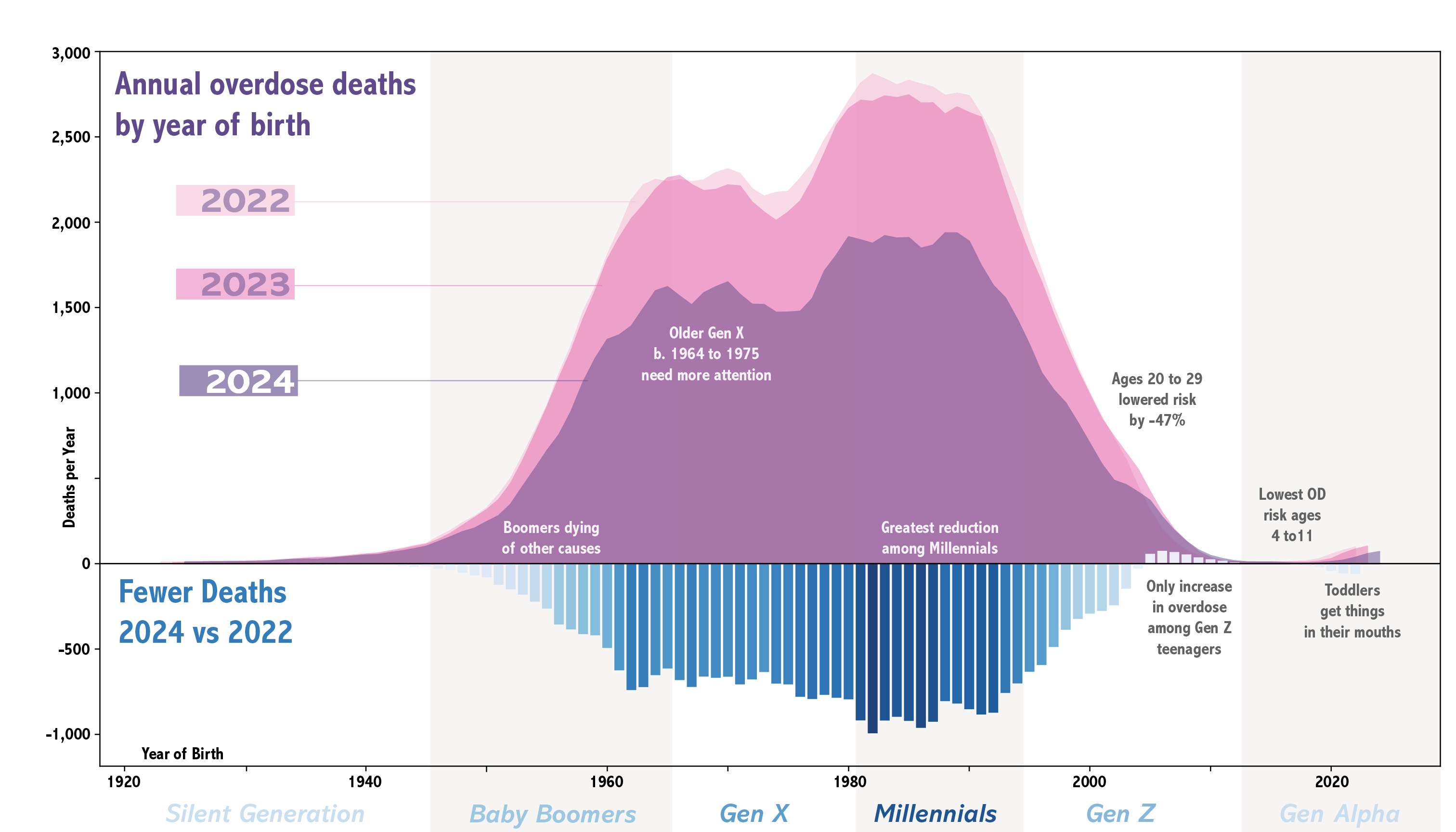
A major reason why Gen Z is turning away from opioids has to do with what they have experienced. 1.4 million kids were there when their aunts, uncles, parents, and grandparents struggled with opioids. Any advertiser will tell you this experience is way more salient than a message campaign. The DEA's "Fentanyl Free" campaign limped into existence in December 2025, right before the holidays. It's a series of radio spots and a logo, but at least it mentions knowing how to access and use naloxone. They seem obsessed with pills, but most OD deaths involve powder. 🤷🏾 This isn't particularly surprising, as DEA has leaned heavily into the one-[fake]-pill-can-kill narrative propagated by their grieving parent advisors whose kids had tragically passed in the previous OD era. The overall effect is that the public education campaign is years out of date. Voices of parents are important, but hinging US policy on anecdotes is not wise; better to have parents that have a broader and more current understanding of drugs and can put their story in context.
International Comparisons
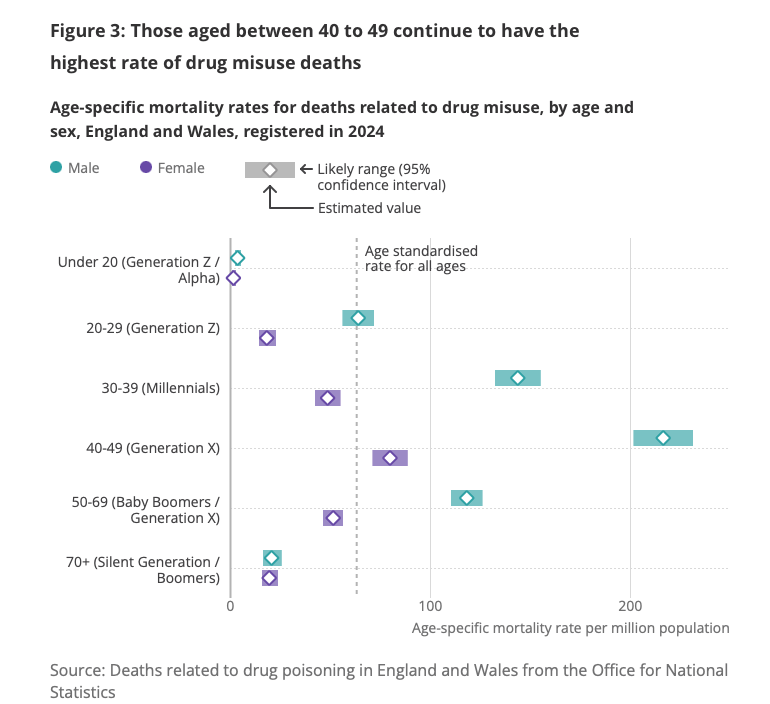
🏴🏴 Looking over at England and Wales, we see the generational breakdown is nearly identical. To make the chart below look the same as the one above, rotate left (counterclockwise) and take the mirror image. 😵💫 Still, the burden of drug overdose deaths is highest in Millennials and Gen X, with Gen Z having markedly less OD deaths.
🇪🇺 And looking at Europe as a whole, we see a remarkably similar pattern in that the younger generation of drug using age (approximately Gen Z) makes up a smaller portion of OD deaths. While there is substantial variation by country due to underlying differences in age distribution (ahem, age-adjusted rates would have been better EUDA!) – the majority of OD death burden is shifted to middle age. In generations past, as a general observation, overdose mortality used to increase in young adulthood (age 20s) and then decline in the 30s and 40s.
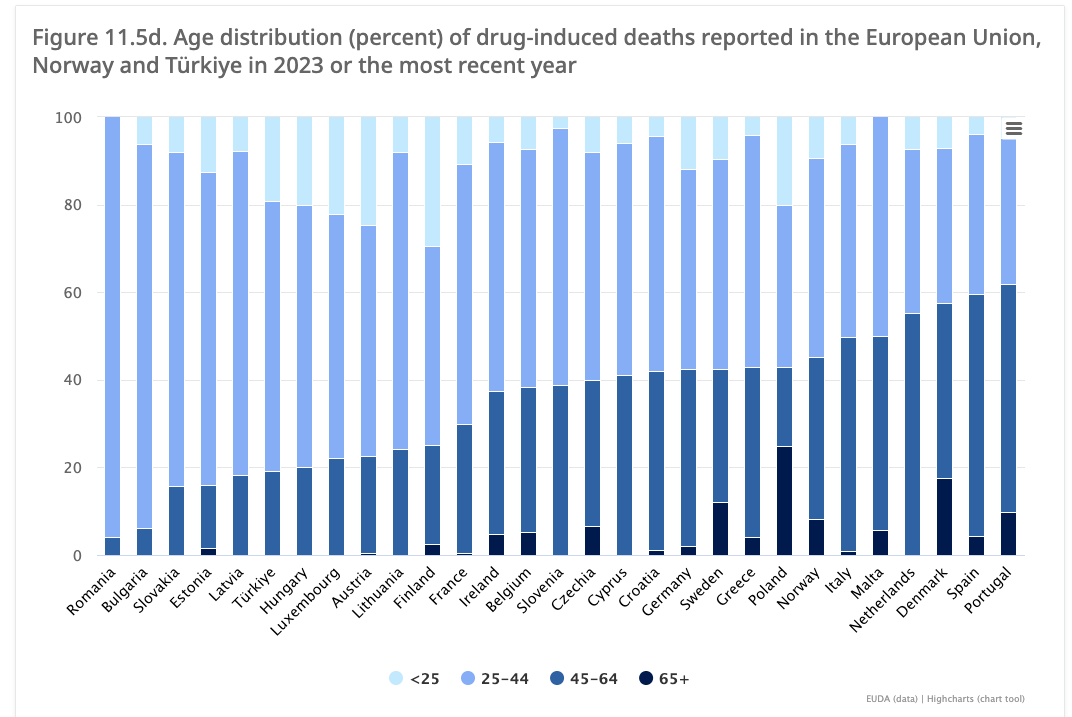
While the emphasis on preventing harms in youth is well-intentioned, the real burden of overdose mortality in the Global North is among the middle aged.
Law Enforcement Data
Back in the US again. In May, as federal law enforcement were diverted into immigration, drug seizures dropped at US international borders. By October, border fentanyl seizure events had reached a new low (n=39). In 2025 for the third year in a row, fentanyl seizures dropped, down -28.6% from 2023.
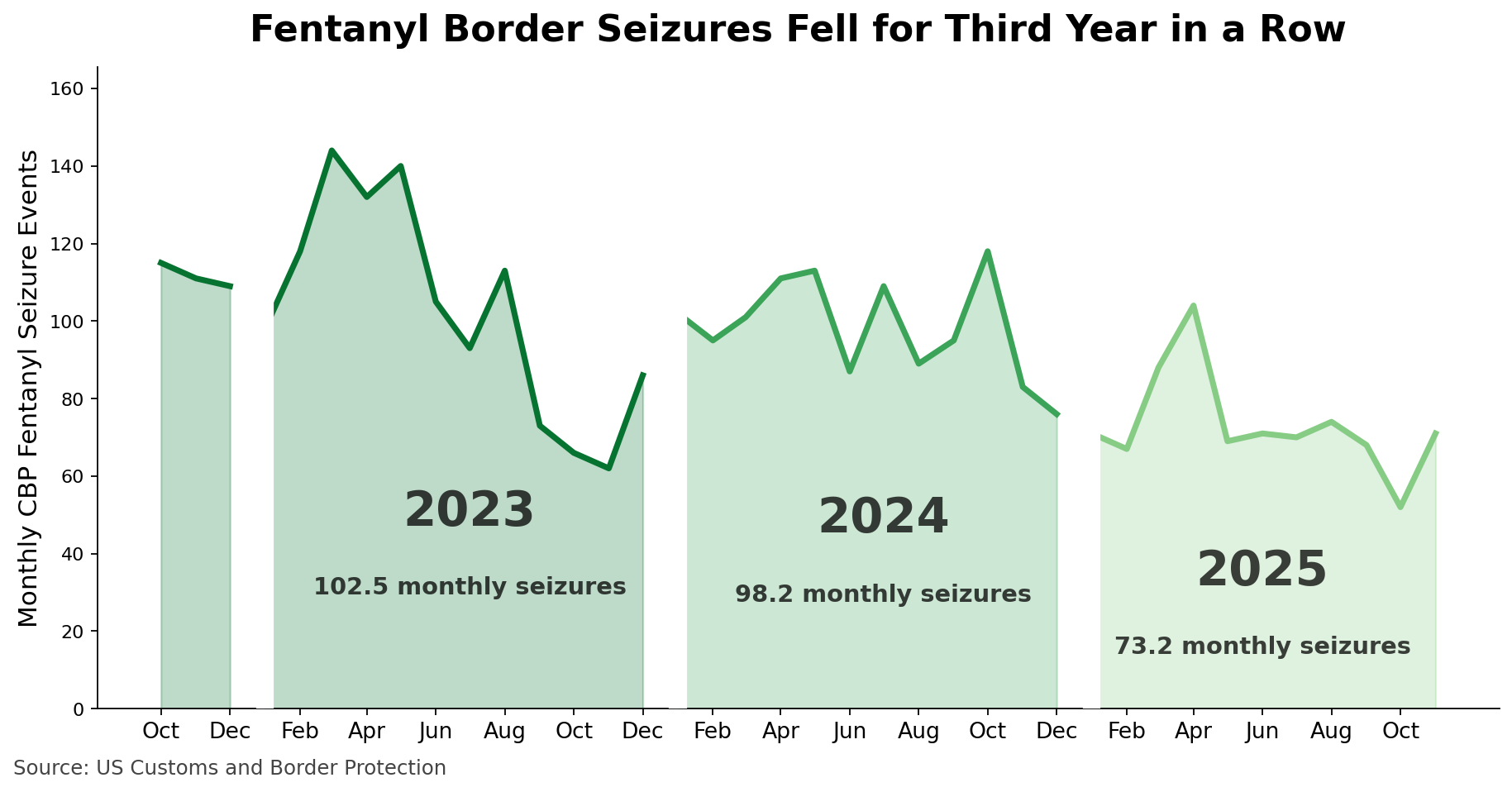
DEA continued to take credit for drops in overdose by touting a decline in the amount of fentanyl per fake pill, attributing success to criminal interdiction. We are left wondering though if border drug seizures themselves an intervention, or are they more of a passive indicator?
Synthesis: countries, time, age
So, what do we make of where we've been? 2024 seems to have been remarkable. Government policy, funding, and priorities were different across these nations. Border seizures in the US fell while OD rates dropped, pointing to an impact from drug supply. Yet, the drugs causing ODs in Scotland were different than in Canada/USA, and Scotland also saw a decline in 2024. What was more consistent across countries however, were changes by generation.
What's the common experience here? (My speculation...) It feels like the restrictions perpetuated by the government response to the COVID pandemic interrupted age-development trajectories and social connectedness. Older generations (Boomers, Gen X, Millennials) turned to opioids to fill some of the longing, because they had had familiarity with those substances from the earlier Rx opioid era. Fentanyl was too strong, but easier to make in the context of a frozen global supply chain. In North America, the timing of the Chineses generic ban on in-country fentanyl manufacturing on the eve of the pandemic (May 2019, see below), and inter-cartel competition in Mexico (partially due to law enforcement-led destabilization of leadership), converged with increased demand to send overdose rates soaring in North America. Gen Z didn't socialize during middle and high school the way their parents had, and did less experimentation with drugs and alcohol. By 2024 it felt like we had moved on from COVID. And some states/provinces had had fentanyl around longer, and/or had better harm reduction and treatment services, and were able to recover (years) faster than nations as a whole. For the first time ever, these services were starting to get meaningful public investment.
In Europe, age/generation disruptions of drug use patterns were similar. On the supply side, the Afghan Taliban's April 2022 ban on opium production created an opening for synthetic opioids, drawing on the North American experience, delivering nitazenes to make up for plummeting supply of heroin, largely skipping over fentanyl. With further disruption of the two largest Mexican cartels in 2024, we are entering an uncertain era.
In the United States, it feels like two drug taste-markets are emerging:
- one emphasizing synthetic opioids, sedatives, methamphetamine, and alcohol for older generations
- one emphasizing cannabis, psychedelics, and plant-grown stimulants catering to Gen Z (and those young-at-heart)
Wastewater Data
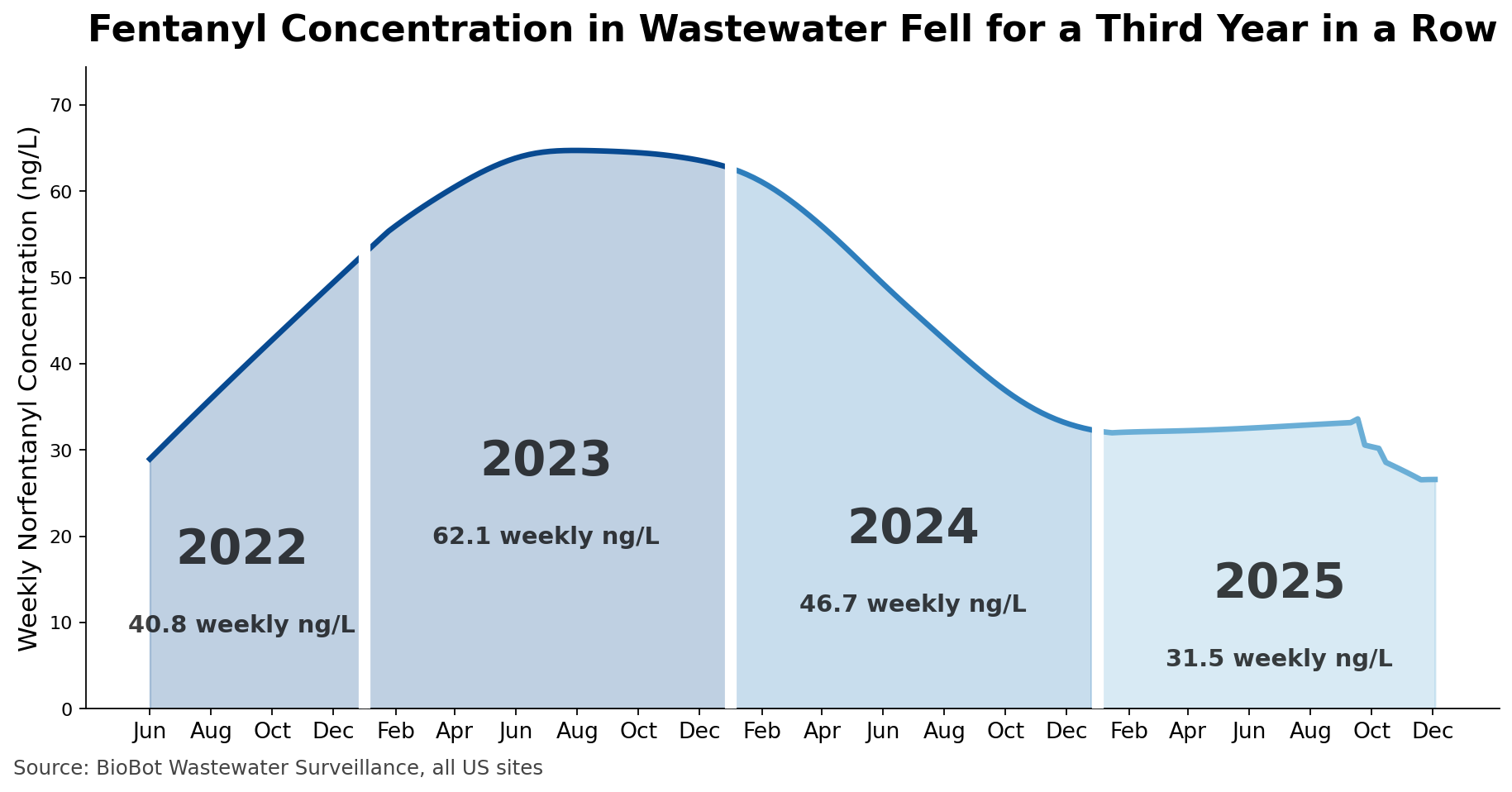
We remain skeptical about BioBot corporation's sewer surveillance data because we don't know their sampling frame and methods, but their national data show similar shape to other data sources (as measured by weekly metabolite norfentanyl concentration). They also seem to imply a sudden drop in September 2025, but again we don't really know their methods.
🍫 At the same time, a drug mixture containing psychoactive substances (theobromine, caffeine, phenethylamine, and anandamide) also decreased in the amount per unit. We are of course talking about chocolate. Less active substance (cocoa butter), more adulterants (vegetable oil, sugar, nuts). Listen to this podcast for causes (hint: drought in West Africa).
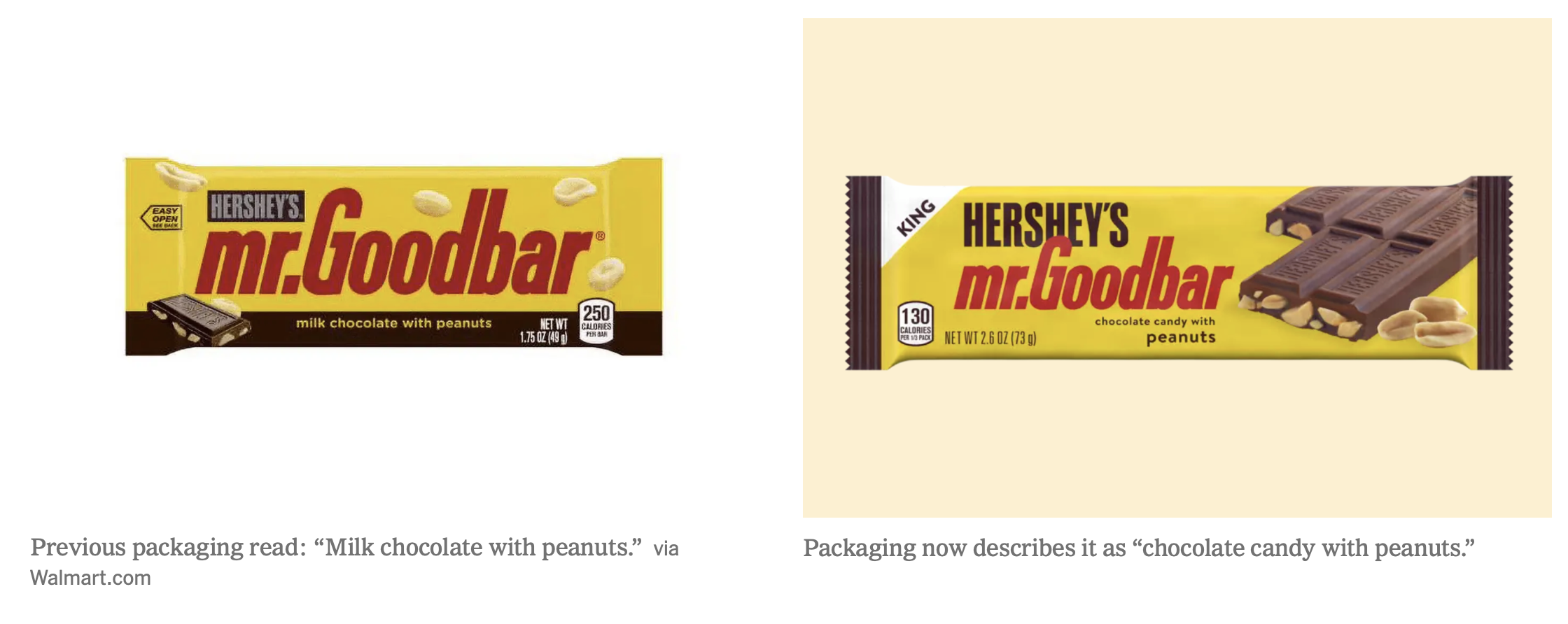
What happens in consumer psychoactive substances is mirrored in the illicit drug supply: Less active ingredient means more adulteration.
Drug Checking Data
Wastewater data cannot tell us if fewer people are using fentanyl, if they are using less, or if using less often. Our fieldwork suggests all three changes in behavior.
Another possibility is that people are not actually getting fentanyl even when they buy it and are expecting it. We looked at samples analyzed using GCMS in our lab (n=8,012) and quantified how often expected-fentanyl samples contained fentanyl in primary abundance.
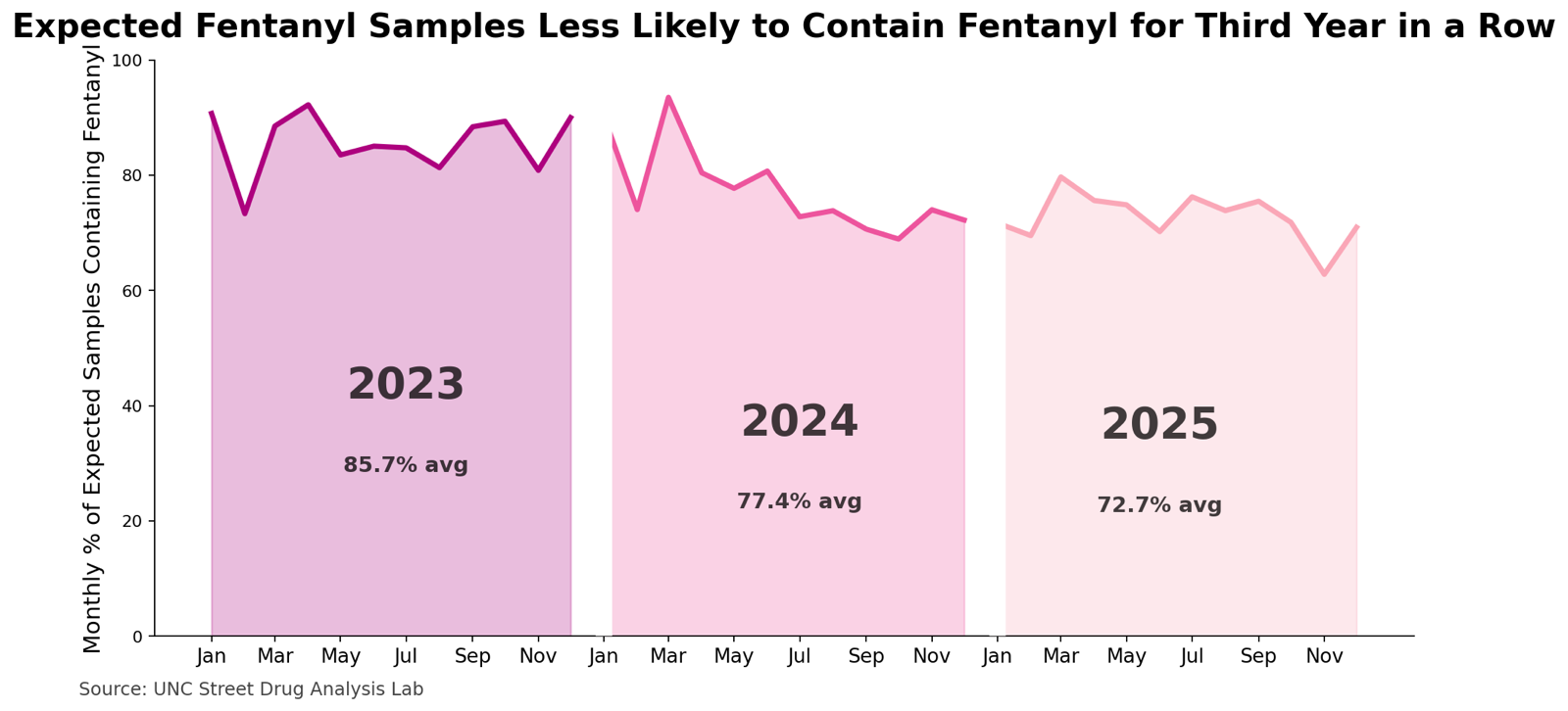
Considered together, across overdose, seizure, wastewater, and drug checking data, the period 2023 to 2025 was notable for the lessening of fentanyl exposure at the population level.
If people aren't getting fentanyl when they expect to have bought fentanyl, then we need to ask what is changing in the drug supply. What is being added instead of fentanyl?
Drug Supply Changes
In 2025, we saw a rising flood of sedatives and numbing agents in the drug supply. Overall reaction to these changes was widespread dissatisfaction. While we are keeping an eye on new classes of synthetic opioids that could replace fentanyl, we are more concerned with medetomidine because it's already replacing fentanyl in some cities; abruptly quitting drug use is suddenly more dangerous than enduring opioid withdrawal.
Sedatives and Numbing Agents
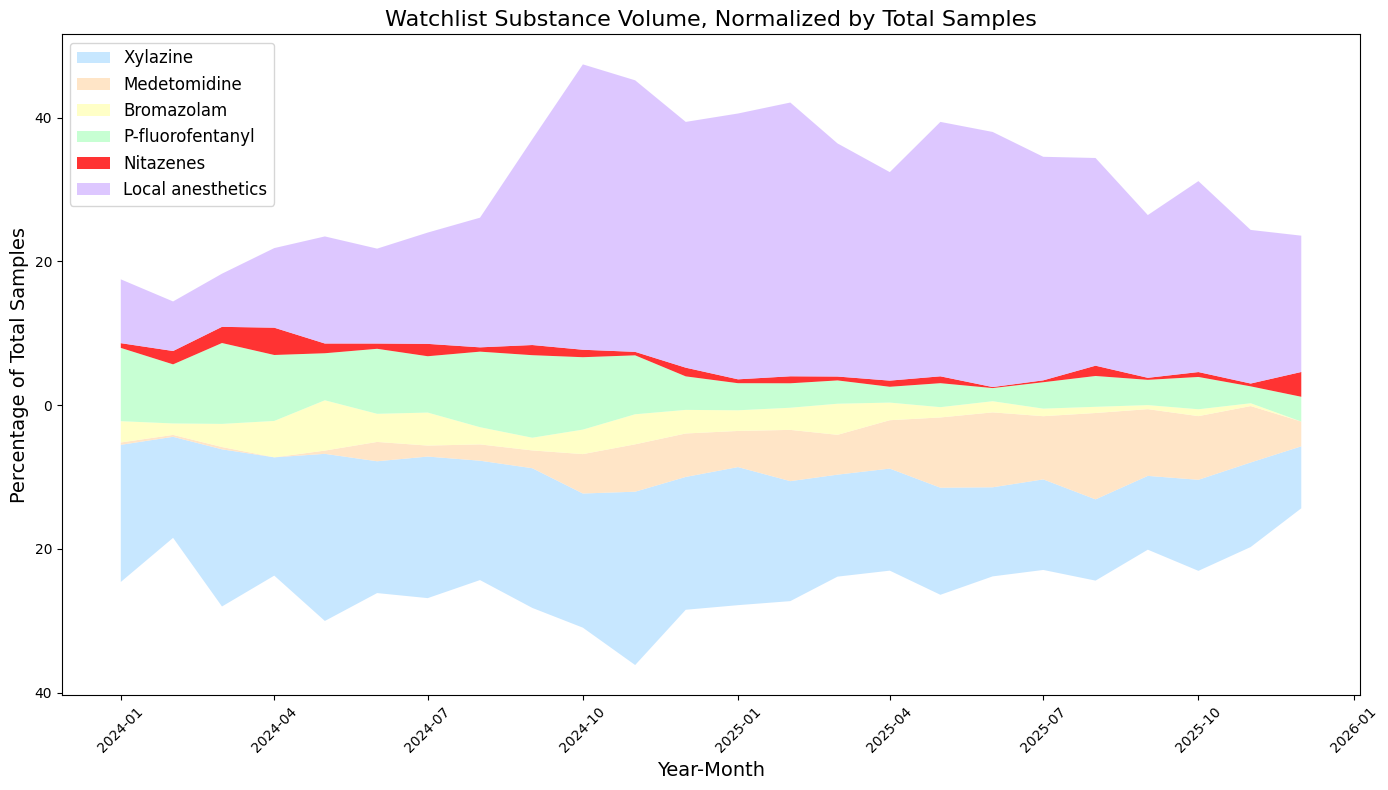
Local anesthetics lidocaine, procaine, and tetracaine (purple in graph), exploded in summer 2024, and continued well into 2025. In fact, we test more samples with local anesthetics than xylazine now! Procaine is also known as Novacain® – the numbing shot you get at the dentist.
Why these numbing agents? We don't know. We speculate there might be some molecular interaction between opioid receptors and local anesthetics that has not been characterized. (Hello, does anyone still work at NIDA?)
Among the fentanyl analogues, we note that in 2025, para-fluorofentanyl (green) was still around but declining, and that this happened before the passage of the HALT Fentanyl Act in July.
Old and new benzos
Bromazolam (a potent benzo, yellow in graph) also decreased in proportion to other fentanyl adulterants, even in the Pacific Northwest where it's been consistent for a few years. In July, Baltimore saw a cluster of non-fatal overdoses involving N-methylclonazepam, an emerging (but still uncommon) potent benzodiazepine. When considered across bromazolam, xylazine, and medetomidine, the influx of sedatives seems a trend likely to continue. Most people who use drugs do not want to be this heavily sedated. In 2025, the unregulated drug supply got noticeably shittier.
Unprepared for medetomidine
At a syringe service program in Pittsburgh, among samples (n=254) we analyzed in 2025, 40% of expected fentanyl samples contained no fentanyl.
(Read that again.)
Instead, 60% of expected fentanyl samples contained medetomidine as a primary drug. Wild! Our lab saw medetomidine heading west, reaching New Mexico and Washington in 2025.
The good news is that unlike its sister molecule xylazine, medetomidine is not a kappa opioid. This means there aren't skin wounds. Medetomidine (also known as dexmedetomidine) is an important human and animal medicine used in hospital anesthesia.
Medetomidine has 3 specific concerns:
1) heavy sedation leaves people vulnerable to theft and assault;
2) strong unpleasant hallucinations;
3) abruptly stopping drug use could lead to high blood pressure requiring a very expensive week-long stay in hospital intensive care.
Medetomidine makes people afraid to stop using drugs because abstinence can be lethal. Alice Bell from Prevention Point Pittsburgh tells us that word is spreading that abruptly stopping dope-with-medetomidine can lead to heart attacks. Their recommendation is not to go to substance use treatment clinics/doctors, but rather to hospitals for detox because the outpatient setting is not equipped to deal with medetomidine withdrawal. Long stays in intensive care are often required in the ICU. And these weeklong stays are expensive. (Medicaid folks, are you listening?)
Medetomidine started replacing xylazine in force around June 2024. By cracking down on (state scheduling) xylazine without simultaneously addressing medetomidine put us in a horrible bind. 🙄 #pwned This isn't just a matter of "oh the drug supply just gets worse" but rather this is a wholly predictable sequence.
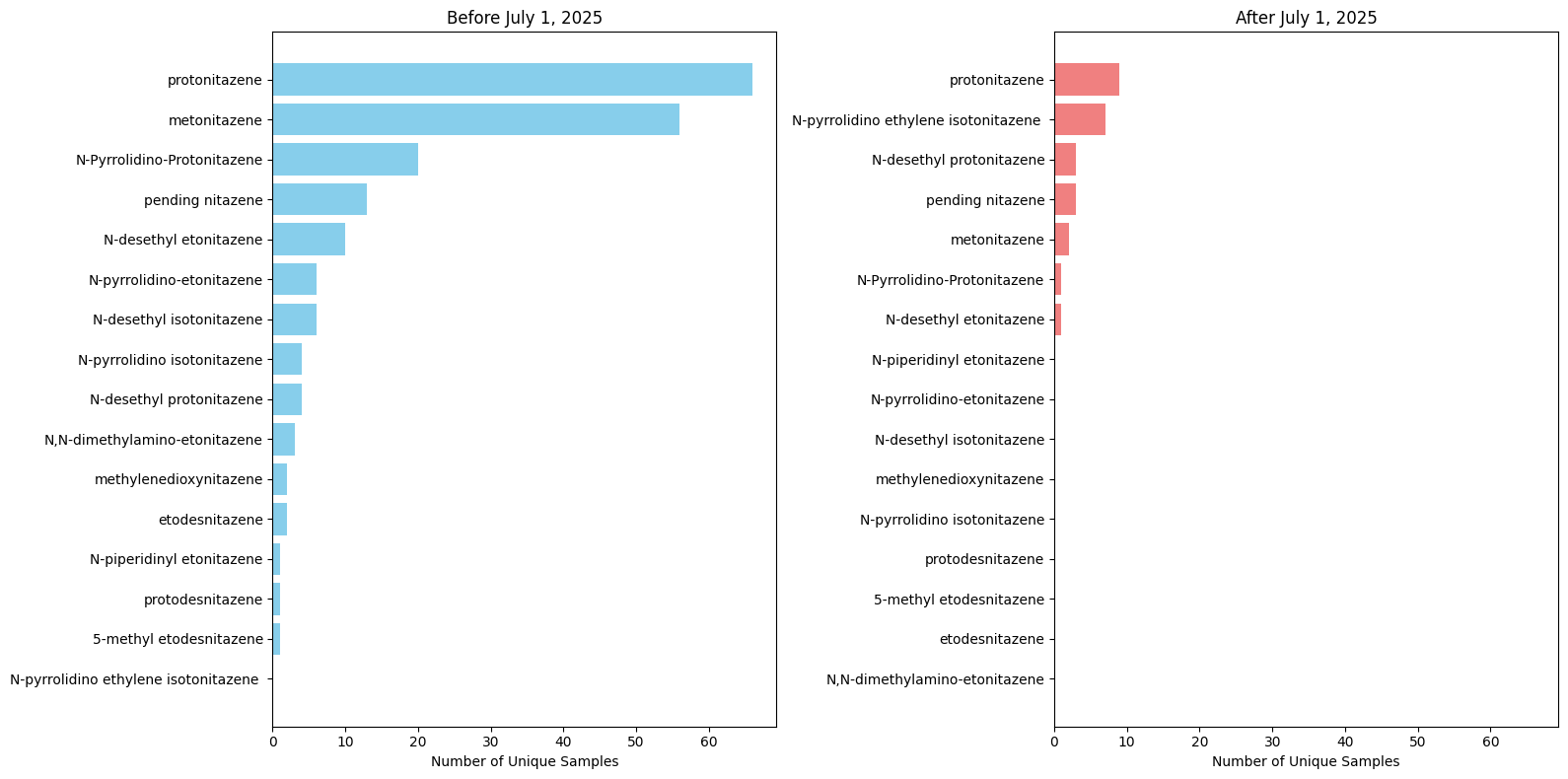
Nitazenes
Nitazenes were another big story, with hyperbolic news coverage overusing the word potency. Among our samples, nitazenes constitute less than 2%. We are keeping an eye on them, but as of December, we aren't seeing a major influx. (See red line in graph above.)
There is a flicker in the line over the summer, corresponding with the Chinese central government generic ban on July 1st. But it's unlikely that our samples would be replaced this quickly, and this wavering may be coincidence. What is clear is that it's not displacing non-opioid sedatives and fentanyl (yet).
But there is an inkling of a subtle change. Both before and after July, protonitazene holds the top spot in terms of frequency within the nitazene class. But metonitazene has dropped from its #2 position. We caution strongly that these are small sample sizes, and that expanded nitazene test strip use may alter what samples we get. At the same time, we saw exactly this kind of market consolidation between fentanyl analogues when the Chinese central government implemented a generic ban in 2019. The variety of fentanyl analogues shrank, and government intervention essentially picked a winner.
(We'd love to hear if our community partners and labs are seeing this shift, including our European colleagues: opioiddatalab@unc.edu. We see less iso species here than Europe, note the new #2 position post-ban.)
New synthetic opioids
Another class of newer synthetic opioids we are watching are the orphines, like this nightmare sample we tested from Michigan containing brorphine. Another in this family is cyclorphine, which showed up in Ontario, Canada and London, England in December.
The other emergent class of synthetic opioids are methadone analogues, like dipyanone and methiodone (IC-26), which we may have had our first detection of from Missouri in October.
In 2025, in the US drug supply, nitazenes, orphines, and methadone analogues are relatively rare. But they introduce new competition to replace fentanyl. All the usual interdiction pressures are in place, now the question is how these molecules will duke it out.
BTMPS on the outs
As we previously noted, the plastic additive bis(2,2,6,6-tetramethyl-4-piperidyl) sebacate looks to be generally on the way out of the US fentanyl supply, albeit slowly. About 20-25% of the fentanyl samples we test still have it though, down from the peak of 40% in Fall 2024.
Why is this happening?
Let's be perfectly clear: The overemphasis on fentanyl is making the drug supply even worse. And, while xylazine made buprenorphine inductions more difficult, the resulting crackdown may be making medetomidine-dope withdrawal dangerous.
Sure, at least some of the sedatives may have less overdose risk, but drug policy targeting fentanyl alone is making 2026 poised to be a hellish year in the drug supply.
We also note that ending de minimis shipping in August may lead to more scrutiny of packages ordered online. This might hit the psychonaut community hard, with fewer shop options the resulting funnel could well reduce the variety of psychedelic substances. On the other hand, smaller shops may emerge and disappear leading to exit scams, chaos, and more discrepancy between what is ordered vs what is received. Caveat emptor, eh?
If you want a better understanding, go to these two must-read articles below. The synthetic cannabinoids are a great example of what happens with classwide "generic" bans. Just like bake-at-home bread, the last time we went through this, we saw semi-finished (ostensibly legal) drug kits in Switzerland to get around the ban, and a shift finished product manufacturing to South Asia.

Bless Their Hearts
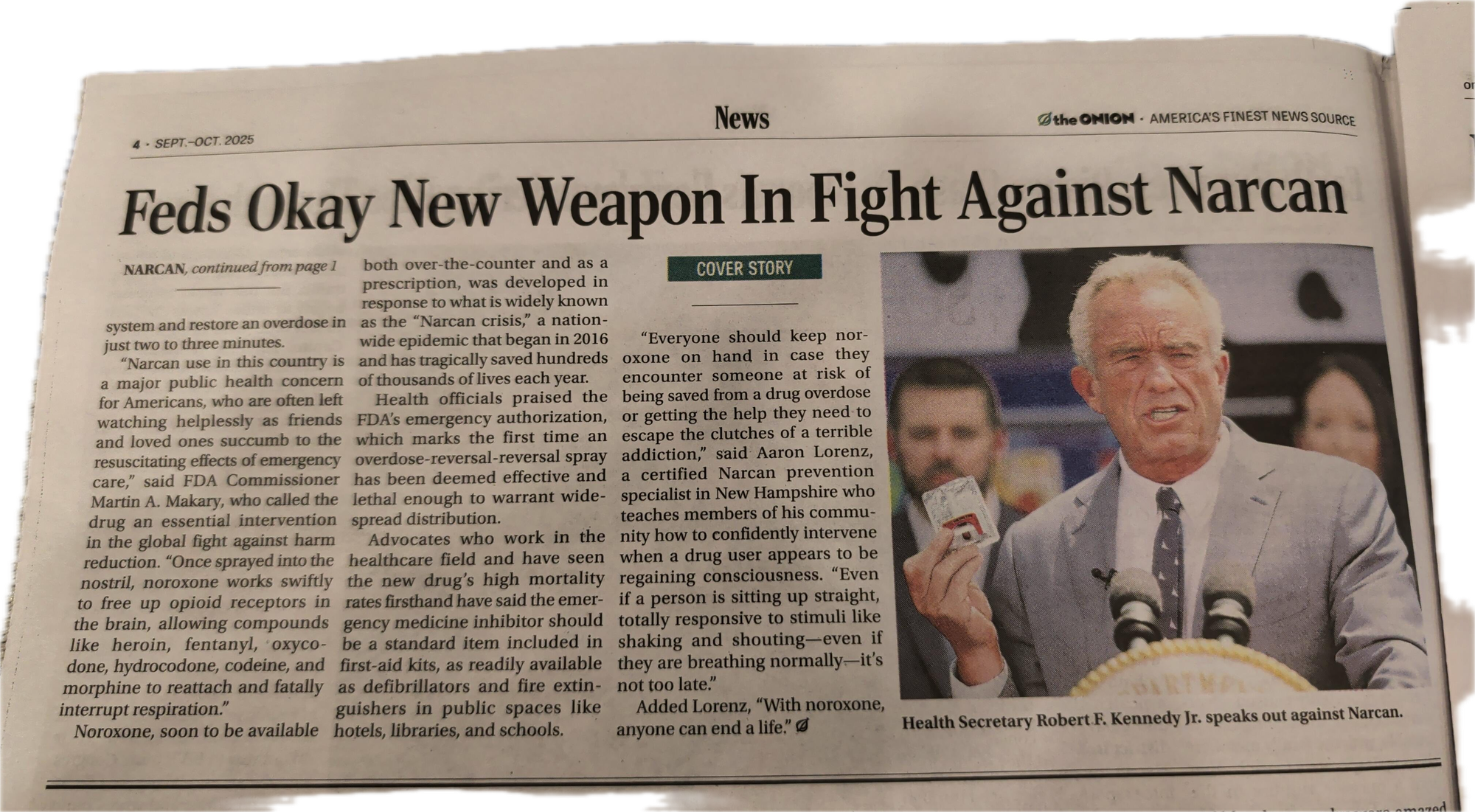
A pricey "herbal infusion" with slick branding, which turned out to be a kava and kratom blend, raised moral outrage in July after a pretty boy TikTok influencer caught a habit. Over the summer, "pink cocaine" (which is not cocaine at all) had a moment, fueled by celebrity follies. News sites like USA Today and CBS provided free advertising to tianeptine manufacturers by featuring their brightly colored packaging as clickbait. Expect interest and demand for tianeptine to flare as irresponsible media coverage boosts this weak opioid with low OD risk and anti-depressant properties.
Meanwhile, the Onion published this:
International Front
The WHO's ECDD rejected a request to down-schedule coca leaf, which has been used religiously and safely for millennia, citing convertibility to cocaine. (A standard that is not consistently applied globally to regulation of other substances.) Some indigenous groups also pointed out that unchecked production could lead to further land invasion, reminding us that over-commercialization and demand in the Global North has tangible consequences.
Former President of the Philippines, Duterte remains in prison, because of extrajudicial killings in the name of the drug war in the early 2000s. Justice takes time.
Drug War Geopolitics
In 2025, the US federal government continued its decades-long game of picking winners and losers among global drug manufacturers. Congress passed HALT Fentanyl Act legislation encouraging the off-shoring of synthetic opioid production away from North America (including Mexico) and towards Asia. Meanwhile, the Executive Branch chose to force the rerouting of cocaine shipments in the Caribbean bound for Europe/Africa, perfectly timed to help cartels raise profits after encountering a European cocaine glut. This beautiful story-map tracks outflows from South America. It is hard to see right now how the United States' synthetic supply of methamphetamine and fentanyl will be impacted by strikes in other regions.
“Standby Mr. President, the drugs are on their way.”
In September, by far the most disturbing development in the Drug War in 2025 was using drugs as a pretext for boat strikes by the United States military. Extrajudicial killings via drone attacks on civilian boats in the Caribbean and Pacific continued through the rest of the year. Strong legal questions have been raised. In December, an Executive Order laid the groundwork for starting another war under the pretense of Weapons of Mass Destruction (WMD). The rhetoric offers a shortcut around evidence, proportionality, and accountability—just as it did in Iraq.
This is political theatre, in the theatre of war. We should pay attention to how this plays out, but it is also a distraction. There are tangible threats in the drug supply completely unrelated to the pending war. Our work of taking care of our own communities needs to continue.
The hard-won gains in reversing the decades-long increase in overdose deaths have largely been through persistent science-driven care. Across the country, I see neighbors taking care of neighbors, removed from the macho national rhetoric spinning on about preventing drug cargo with walls and drones and warships. In rural communities and urban clusters, nobody wise is sitting around waiting for airstrikes on boats in the Caribbean. Instead, we take care of our own.
State of harm reduction
By one measure, harm reduction is flourishing globally: 112 countries explicitly endorse harm reduction in national policies. On the other hand, 92% of harm reduction advocates say services in their country are under threat, with 62% describing the threat as high or critical.
HRI puts this beautifully:
Across the world, programmes are shrinking or closing. Outreach teams have been cut. Supplies are running out. Communities that rely on harm reduction to stay alive are facing impossible choices.
But there is also hope and determination.
We documented remarkable resilience:
• Countries with domestic funding have protected essential services.
• Peer-led networks have stepped in where formal systems have collapsed.
• Organisations have pooled limited resources to keep people safe, supported, and alive.
This update makes one thing clear: harm reduction works. But only if it’s funded.
In the US, harm reduction notched a smirking victory when Indivior stopped marketing (not selling) nalmefene nasal spray, the unnecessary and financially unviable (expensive) competitor to generic naloxone.
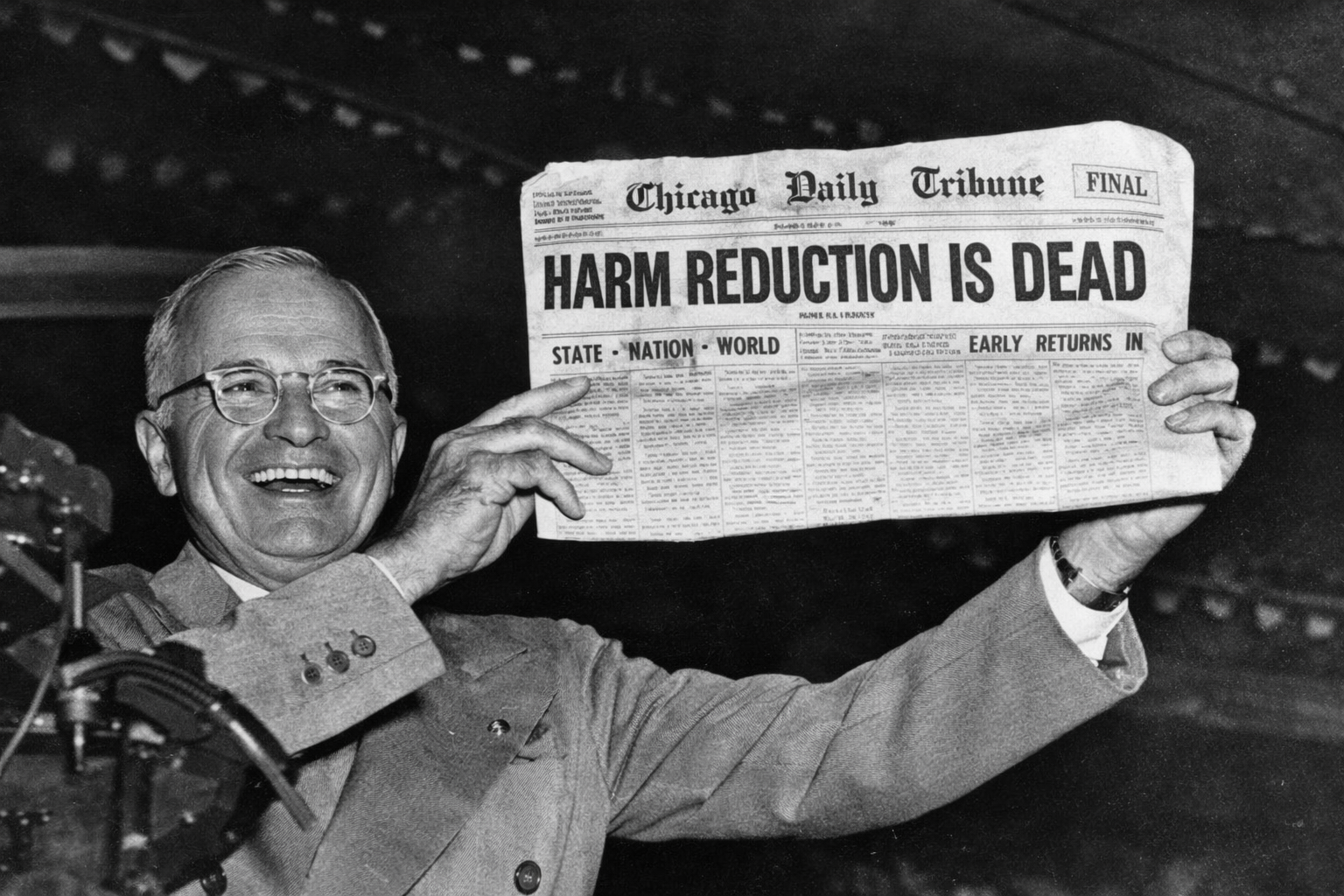
An Executive Order in July took aim at safe consumption spaces, or overdose prevention centers. In September, HHS tried to prematurely declare harm reduction dead, through letters issued via CDC and SAMHSA. There is a huge harm reduction workforce that is not going anywhere. Sure, many orgs chose to scrub those two words "harm reduction" from their websites. It erodes our collective identity, but doesn't diminish our resolve to see our communities thrive.
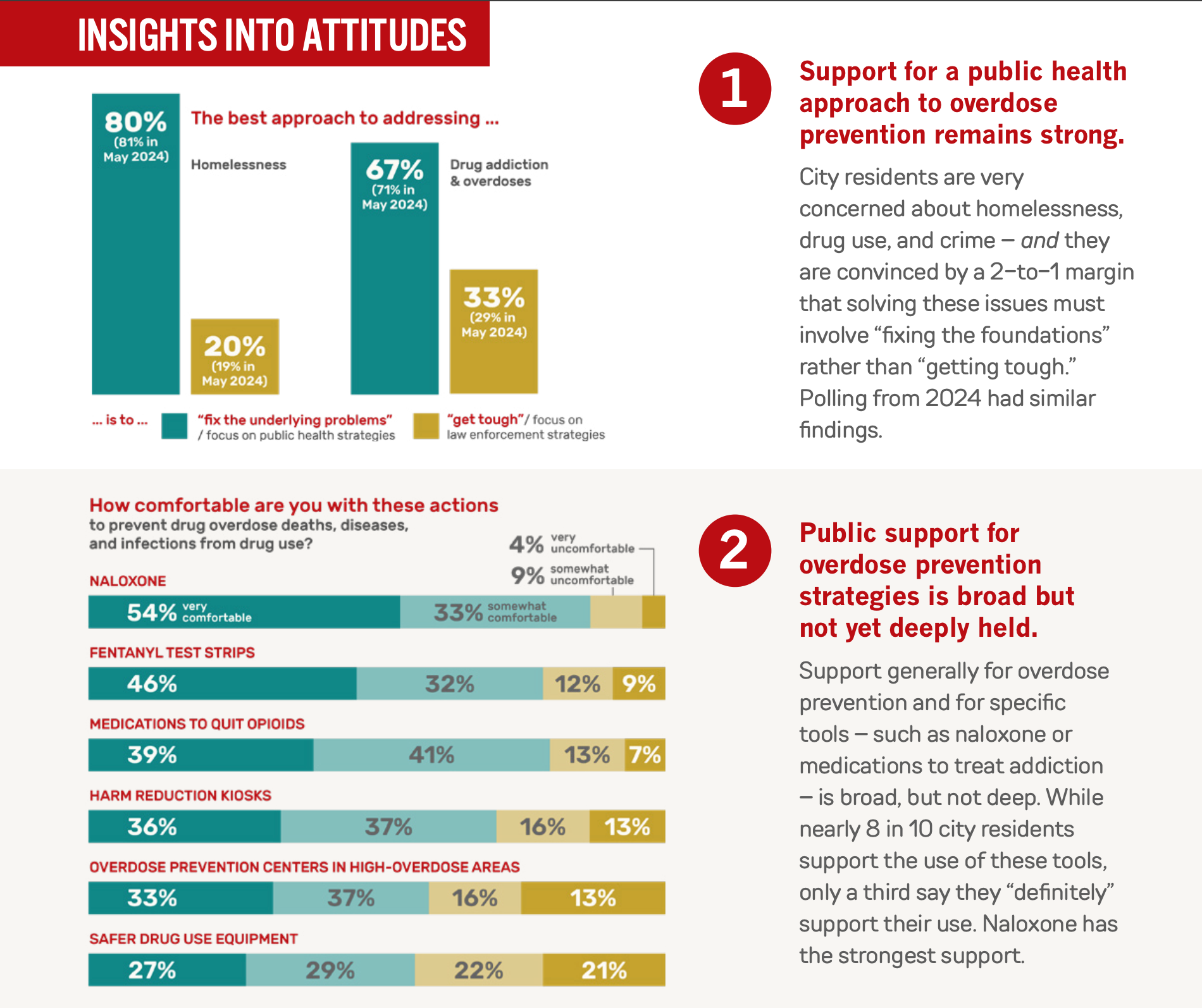
But the anti-harm reduction stance is also tone-deaf. There are millions of Americans whose lives have been touched by close relatives struggling with addiction. (Bookmark this excellent messaging playbook.) Polling in 2025 revealed that compassion and second chances are supported by wide segments of the population.
It is surprising then that the politicians are taking an axe to health insurance funding, paring back eligibility for Medicaid, introducing work requirements and paperwork (track it here). Reducing access to drug treatment is exactly the wrong direction from where we need to go. We have a moment, in 2026, to make real and lasting changes. Let's not squander it.
What these federal actions do is effectively reduce funding. And this is where opioid settlements come in.
Opioid Settlements
Nearly three decades after the initial crimes, the settlement against Purdue Pharma's Sackler family was finally approved in November; let's hope it sticks this time.
Waste, Fraud, Abuse, Mismanagement
Some states are seem to be spending opioid settlements well. But in reality NO state is across the board good, with some states doing better at the county level but not the state level.
But county spenders were getting duped by unscrupulous vendors in damn near every state. Y'all need to get it together, and not be scammed.
Drones in Arizona. Millions of dollars on disposal pouches (California, Colorado, Connecticut, Indiana, Iowa, and elsewhere). Dog food and vet bills for K9 units. An ice rink in Kentucky. Handheld drug analysis devices that don't work. Body cameras in Michigan. An office move, fiber optic cables, and shelving in Mississippi. (Seriously, $12,000 for an office shelving system!) $7,500 for T-shirts in Missouri. Hundreds of thousands of dollars for concerts in New Jersey. Plenty of non-opioid activity in Pennsylvania. A padded cell in South Dakota. A camera upgrade in Tennessee. Drones in West Virginia. Overpriced "fentanyl proof" gloves in Wisconsin.
Stay tuned for a major report on this early next year, and check out the list being tracked in real-time here:

There are things that are less likely to get federal funding now, like syringe service programs, pipes, overdose prevention centers, and housing-first programs. These are things that settlement funds should prioritize over other things.
Marijuana: Is this the year?
In November, Congress quietly closed a loophole that allowed small amounts of quasi-legal delta-9 THC retail sales in states that hadn’t legalized weed. Will it be back to the unpredictable sensations from Delta-8? Will there be have and have-not states? Are dispensaries expected to become pharmacies? Mobilization of small businesses will be worth watching.
Wildcard in December: the perennial promise of cannabis legalization was batted around, but this time via Executive Order putting it in Schedule III. It is supposed to "clear the way for research" and medical purposes. An improvement from Schedule I, but far from effective regulation. Unclear how far this is going to go. Impacts on patient access would not be surprising, meaning opportunity for black markets. “Wellness influencers” and ketamine are a cautionary tale, including speculation of what Elon Musk is on.
Just gonna say this because it needs repeating: Marijuana in 2025 did not show signs of being contaminated with fentanyl.
Housing: Elephant in the Room
So much of public sentiment (and therefore policy) about drugs is fueled by what can be seen from a car window. Housing insecurity, chaotic public drug use, even the smell of weed on the sidewalk... these are the things that always come up first when we talk about our work to normies. (And kids mistakenly taking pills "laced" with fentanyl.)
Prevention works, but it also renders our efforts invisible. We are on the precipice of undoing years of painstaking good work in reducing drug harms. From an HIV outbreak in Maine to ending the housing-first program in Utah, getting folks into housing is essential to ending long-term drug harms. If you want to get caught up on the science of homelessness and what we can do to truly alleviate the problem, start following Dr. Margot Kushel.
Data landscape
Our understanding of national overdose numbers took a major hit when the formulae to calculate CDC provisional and predicted overdose deaths were changed in February with no announcement. In addition to updating the baseline model, the reporting lag is supposed to be now 4 months instead of 6. The gag order on CDC officials from speaking is harmful. We need the deets! The jury is still out on the revised methodology, but we're looking into it.
We also saw wild applications of AI to monitor people's drug use, like this example from Florida. Sewer surveillance (wastewater testing) for drugs also expanded, driven by for-profit companies and NIDA, with summer partygoers in Nantucket getting called out for using blow.
What would it take to harness the ingenuity of the private sector to improve government data collection? Here’s our shortlist of four things to keep an eye on as info sources shift. In fact the whole January issue of American Journal of Public Health is dedicated to regaining public trust.
Finally, it wouldn't be a 2025 retrospective unless we mentioned AI. 🤖🤣
Under the banner of the war on drugs, governments are quietly expanding AI-driven surveillance tools—facial recognition, predictive policing algorithms, social-media monitoring, license-plate readers, and automated report generation—often with minimal public oversight or evidence of effectiveness, raising serious civil liberties concerns about privacy and transparency. The Brennan Center is doing excellent work in this area.
Here comes 2026
With the successes of 2024 now clear, and our ability to hold steady in 2025, we face a tremendous opportunity in 2026. There are more people engaged with harm reduction than ever before. And yet the threats from an unregulated drug supply, reduced federal funding, and outdated rhetoric are impediments. We have a once-in-multiple-generations chance, right here, right now. Let's not squander it.